

Abstract
Introduction
Multiple myeloma (MM) causes lytic bone lesions, osteopenia, and fractures, which increase the morbidity of MM patients. Results from small previous studies have indicated that fractures in MM have a negative effect on survival.
Aims
The aim of the study was to evaluate the impact of fractures on survival in MM patients diagnosed in Sweden in the years 1990-2013. Furthermore, to analyze the effect of bone fractures at MM diagnosis on subsequent survival.
Methods
Patients diagnosed with MM in 1990-2013 were identified from the Swedish Cancer Registry. Information on date of birth, diagnosis, and death were collected from the Registry of Total Population. Information on all fractures were retrieved from the Swedish Patient Registry. Cox regression model was used with fractures as time-dependent variables. The effect of fractures on survival was assessed for any fracture or a subtype of fracture (a specific bone fracture or ICD-coded pathologic fracture). Either first fracture or the first subtype of fracture was used in the analysis. The effect of a fracture at MM diagnosis (within 30 days before or 30 days after MM diagnosis) on survival was also estimated using a Cox regression model. All models were adjusted for age, sex, time of diagnosis, and previous fractures.
Results
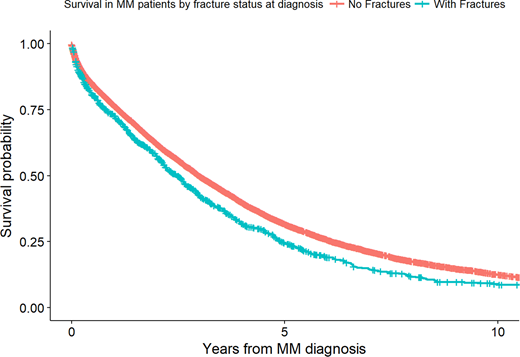
A total of 14,008 patients were diagnosed with MM in the study period. A total of 4,141 (29.6%) patients developed a fracture including fractures that occurred within a year before MM diagnosis and thereafter. Hereof 2,893 (20.7%) patients developed a fracture after MM diagnosis. The risk of death was significantly increased for patients that developed a fracture after the time of MM diagnosis with a hazard ratio (HR) of 2.00 (95% confidence interval (CI) 1.91-2.10) for all fractures combined. The risk of death was significantly increased for patients that developed all subtypes of fractures after MM diagnosis except ankle fractures. The risk of death was significantly increased for patients that developed pathologic fractures (HR=2.17; 95% CI 2.03-2.32), vertebral fractures (HR=1.73; 95% CI 1.61-1.87), hip fractures (HR=1.99; 95% CI 1.82-2.18), femoral fractures (HR=2.62; 95% CI 2.32-2.98), humerus fractures (HR=2.57; 95% CI 2.32-2.86), forearm fractures (HR=1.24; 95% CI 1.05-1.46), and rib fractures (HR=1.52; 95% CI 1.31-1.77), but not for ankle fractures (HR 1.07; 95% CI 0.79-1.44). A total of 942 (6.7%) of all MM patients were diagnosed with a fracture within 30 days before or 30 days after MM diagnosis. The patients with a fracture at diagnosis were at a significantly increased risk of death compared to those without (HR 1.31; 95% CI 1.21-1.41; Figure)
Conclusions
Our large population-based study, including over 14,000 patients diagnosed with MM in Sweden in the years 1990-2013, showed that MM patients that developed a fracture after the time of diagnosis were at twofold increased risk of dying compared to MM patients without a fracture. Furthermore, MM patients with a fracture at diagnosis had a 30% higher risk of dying compared to patients without a fracture. Our results indicate that fractures in MM reflect a more advanced disease at diagnosis and stress the importance of managing MM bone disease in all MM patients.
Landgren:Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Consultancy; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Consultancy; Celgene: Consultancy, Research Funding; Amgen: Consultancy, Research Funding.

